Introduction: Lymphoepithelial cyst (LEC) of vallecula is an uncommon benign lesion. Cysts in vallecula can present with odynophagia, dysphagia, dysphonia and stridor. Many times, they can be asymptomatic. They can pose difficulty in intubation. On endoscopic evaluation it may mimic the appearance of a lipoma because of its yellowish appearance. Management of this requires adequate visualization and instrumentation. It can be done under endoscopic guidance or laryngoscopy by using cold steel method or laser or coblator. Because of rarity of the lesion, case has been reported. Case report: A 54-year-old male presented with odynophagia. An upper gastrointestinal endoscopy done by gastroenterologist revealed a mass in left vallecula and was then referred to otorhinolaryngologist. Excision was done using coblator under endoscopic guidance under general anaesthesia. Coblator enabled precise excision with adequate hemostasis without multiple repeated instrumentations. Histopathology confirmed it as a Lymphoepithelial cyst. Patient was discharged the next day with oral antibiotics and analgesics and at follow up was asymptomatic and endoscopic examination showed a well healed site of the lesion. Conclusion: Lymphoepithelial cyst of vallecula is a rare lesion. It can be excised using coblator under endoscopic guidance with advantage of having better precision, reduced bleeding, faster recovery compared to conventional methods. This technique can be used for other vallecular benign lesions as well.
| Published in | Advances in Surgical Sciences (Volume 13, Issue 1) |
| DOI | 10.11648/j.ass.20251301.11 |
| Page(s) | 1-4 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Lymphoepithelial Cyst, Vallecula, Coblator, Endoscopy
LEC | Lymphoepithelial Cyst |
| [1] | Elakhiri, Mohammed & Sahli, Mohamed & Tayane, Mossab & Aljalil, Abdelfattah & Ammar, Haddou & Darouassi, Youssef. (2021). Lymphoepithelial Cyst of the Vallecules: A Case Report and Literature Review. Saudi Journal of Medicine. 6. 60-62. |
| [2] | Romak, Jonathan & Olsen, Steven & Koch, Cody & Ekbom, Dale. (2010). Bilateral Vallecular Cysts as a Cause of Dysphagia: Case Report and Literature Review. International journal of otolaryngology. 2010. 697583. |
| [3] | Bae HM, Yoon JR, Yoo JH, Han YJ, Park YJ. A vallecular cyst in a patient with deep neck infection causing difficult airway management. Korean J Anesthesiol. 2014 Dec; 67(Suppl): S21-2. |
| [4] | Nanda C. A Rare Case of Unanticipated Difficult Intubation Due to a Vallecular Cyst. J Card Crit Care TSS. 2024; 8: 252-3. |
| [5] | Gaxa, Luvo & Hlatshwayo, Bafana & Magaroleng, Hendry & Modishi, (2015). Vallecular cyst. Case Reports International. 4. 6-10. |
| [6] | Lahiri AK, Somashekar KK, Wittkop B, Ayshford C. Large Vallecular Masses; Differential Diagnosis and Imaging Features. J Clin Imaging Sci. 2018 Jun 28; 8: 26. |
| [7] |
Puneeth PJ, Balushi F, Gandhi S. Vallecular Cyst: 10 Years Experience and Review of the Literature. Indian J Otolaryngol Head Neck Surg. 2023 Jun; 75(2): 492-495.
https://doi.org/10.1007/s12070-022-03319-3 Epub 2022 Dec 11. |
| [8] |
Torun MT, Seçkin E, Tuncel Ü, Kılıç C, Özkan Ö. A Rare Entity: Adult Asymptomatic Giant Vallecular Cyst. Case Rep Otolaryngol. 2015; 2015: 723420.
https://doi.org/10.1155/2015/723420 Epub 2015 Nov 24. |
| [9] | Sykara M, Ntovas P, Kalogirou EM, Tosios KI, Sklavounou A. Oral lymphoepithelial cyst: A clinicopathological study of 26 cases and review of the literature. J Clin Exp Dent. 2017 Aug 1; 9(8): e1035-e1043. |
| [10] | Yuce Y, Uzun S, Aypar U. Asymptomatic vallecular cyst: case report. Braz J Anesthesiol. 2013 Sep-Oct; 63(5): 419-21. |
| [11] | George C, Martin A, Osahan NM, Liddle D. Anesthetic and Surgical Management of Mucoid Retention Cyst in the Vallecular Region: An Airway Challenge. J Indian Assoc Pediatr Surg. 2018 Oct-Dec; 23(4): 234-235. |
| [12] |
Vijayanand H, Mudhol RS, Patil PH, Maheswaran M. Innovative surgical management of large vallecular cysts. Indian J Otolaryngol Head Neck Surg. 2009 Jun; 61(2): 147-9.
https://doi.org/10.1007/s12070-009-0055-z Epub 2009 Jun 14. |
| [13] | Hoang, T. M., & Kim, B. B. (2015). A Case Report of a Vallecular Cyst and Literature Review. Journal of Oral and Maxillofacial Surgery, 73(9), 1766.e1–1766.e4. |
| [14] | Tan KS, Jalaluddin WMS. Lipoma of vallecula-a case report. BJR Case Rep. 2016 Jul 28; 2(3): 20150460. |
| [15] | Ting LKN, Idris A, Mat Baki M. Rare cause of voice muffling: pyogenic vallecular cyst. BMJ Case Rep. 2022 Sep 15; 15(9): e250615. |
| [16] | Nathani N, Verma PC, Sharma MP. Cyst vallecula unusual presentation. Indian J Otolaryngol Head Neck Surg. 2006 Oct; 58(4): 410-1. |
| [17] |
Suzuki J, Hashimoto S, Watanabe K, Takahashi K. Congenital vallecular cyst in an infant: case report and review of 52 recent cases. J Laryngol Otol. 2011 Nov; 125(11): 1199-203.
https://doi.org/10.1017/S0022215111001368 Epub 2011 Jun 14. |
| [18] |
Prowse S, Knight L. Congenital cysts of the infant larynx. Int J Pediatr Otorhinolaryngol. 2012 May; 76(5): 708-11.
https://doi.org/10.1016/j.ijporl.2012.02.025 Epub 2012 Feb 28. |
| [19] |
Kayhan FT, Kaya KH, Koc AK, Altintas A, Erdur O. Transoral surgery for an infant thyroglossal duct cyst. Int J Pediatr Otorhinolaryngol. 2013 Sep; 77(9): 1620-3.
https://doi.org/10.1016/j.ijporl.2013.07.007 Epub 2013 Aug 2. |
| [20] |
Gonik N, Smith LP. Radiofrequency ablation of pediatric vallecular cysts. Int J Pediatr Otorhinolaryngol. 2012 Dec; 76(12): 1819-22.
https://doi.org/10.1016/j.ijporl.2012.09.008 Epub 2012 Sep 26. |
APA Style
Bhyranna, M. G., Devaraj, D. D., Munishwara, T. G., Sugantharajan, S. K., Bhat, V. S. (2025). Management of Lymphoepithelial Cyst of Vallecula by Coblator, a Case Report and Literature Review. Advances in Surgical Sciences, 13(1), 1-4. https://doi.org/10.11648/j.ass.20251301.11
ACS Style
Bhyranna, M. G.; Devaraj, D. D.; Munishwara, T. G.; Sugantharajan, S. K.; Bhat, V. S. Management of Lymphoepithelial Cyst of Vallecula by Coblator, a Case Report and Literature Review. Adv. Surg. Sci. 2025, 13(1), 1-4. doi: 10.11648/j.ass.20251301.11
AMA Style
Bhyranna MG, Devaraj DD, Munishwara TG, Sugantharajan SK, Bhat VS. Management of Lymphoepithelial Cyst of Vallecula by Coblator, a Case Report and Literature Review. Adv Surg Sci. 2025;13(1):1-4. doi: 10.11648/j.ass.20251301.11
@article{10.11648/j.ass.20251301.11,
author = {Munishwara Galigekere Bhyranna and Deeksha Devaki Devaraj and Thrupthi Galigekere Munishwara and Swarna Kamala Sugantharajan and Vinay Shridhar Bhat},
title = {Management of Lymphoepithelial Cyst of Vallecula by Coblator, a Case Report and Literature Review
},
journal = {Advances in Surgical Sciences},
volume = {13},
number = {1},
pages = {1-4},
doi = {10.11648/j.ass.20251301.11},
url = {https://doi.org/10.11648/j.ass.20251301.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ass.20251301.11},
abstract = {Introduction: Lymphoepithelial cyst (LEC) of vallecula is an uncommon benign lesion. Cysts in vallecula can present with odynophagia, dysphagia, dysphonia and stridor. Many times, they can be asymptomatic. They can pose difficulty in intubation. On endoscopic evaluation it may mimic the appearance of a lipoma because of its yellowish appearance. Management of this requires adequate visualization and instrumentation. It can be done under endoscopic guidance or laryngoscopy by using cold steel method or laser or coblator. Because of rarity of the lesion, case has been reported. Case report: A 54-year-old male presented with odynophagia. An upper gastrointestinal endoscopy done by gastroenterologist revealed a mass in left vallecula and was then referred to otorhinolaryngologist. Excision was done using coblator under endoscopic guidance under general anaesthesia. Coblator enabled precise excision with adequate hemostasis without multiple repeated instrumentations. Histopathology confirmed it as a Lymphoepithelial cyst. Patient was discharged the next day with oral antibiotics and analgesics and at follow up was asymptomatic and endoscopic examination showed a well healed site of the lesion. Conclusion: Lymphoepithelial cyst of vallecula is a rare lesion. It can be excised using coblator under endoscopic guidance with advantage of having better precision, reduced bleeding, faster recovery compared to conventional methods. This technique can be used for other vallecular benign lesions as well.
},
year = {2025}
}
TY - JOUR T1 - Management of Lymphoepithelial Cyst of Vallecula by Coblator, a Case Report and Literature Review AU - Munishwara Galigekere Bhyranna AU - Deeksha Devaki Devaraj AU - Thrupthi Galigekere Munishwara AU - Swarna Kamala Sugantharajan AU - Vinay Shridhar Bhat Y1 - 2025/03/31 PY - 2025 N1 - https://doi.org/10.11648/j.ass.20251301.11 DO - 10.11648/j.ass.20251301.11 T2 - Advances in Surgical Sciences JF - Advances in Surgical Sciences JO - Advances in Surgical Sciences SP - 1 EP - 4 PB - Science Publishing Group SN - 2376-6182 UR - https://doi.org/10.11648/j.ass.20251301.11 AB - Introduction: Lymphoepithelial cyst (LEC) of vallecula is an uncommon benign lesion. Cysts in vallecula can present with odynophagia, dysphagia, dysphonia and stridor. Many times, they can be asymptomatic. They can pose difficulty in intubation. On endoscopic evaluation it may mimic the appearance of a lipoma because of its yellowish appearance. Management of this requires adequate visualization and instrumentation. It can be done under endoscopic guidance or laryngoscopy by using cold steel method or laser or coblator. Because of rarity of the lesion, case has been reported. Case report: A 54-year-old male presented with odynophagia. An upper gastrointestinal endoscopy done by gastroenterologist revealed a mass in left vallecula and was then referred to otorhinolaryngologist. Excision was done using coblator under endoscopic guidance under general anaesthesia. Coblator enabled precise excision with adequate hemostasis without multiple repeated instrumentations. Histopathology confirmed it as a Lymphoepithelial cyst. Patient was discharged the next day with oral antibiotics and analgesics and at follow up was asymptomatic and endoscopic examination showed a well healed site of the lesion. Conclusion: Lymphoepithelial cyst of vallecula is a rare lesion. It can be excised using coblator under endoscopic guidance with advantage of having better precision, reduced bleeding, faster recovery compared to conventional methods. This technique can be used for other vallecular benign lesions as well. VL - 13 IS - 1 ER -
Department of Ear Nose Throat, Siddaganga Medical College and Research Institute, Tumakuru, Karnataka, India
Department of Ear Nose Throat, Indira Gandhi Institute of Child Health, Bangalore, Karnataka, India
Bangalore Medical College and Research Institute, Bangalore, Karnataka, India
Department of Pathology, Cytecare Hospital, Bangalore, Karnataka, India
Department of Ear Nose Throat, Siddaganga Medical College and Research Institute, Tumakuru, Karnataka, India
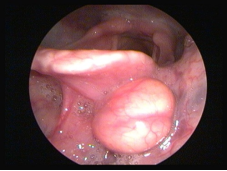
Figure 1. Endoscopic view showing a yellowish mass with a smooth surface in the left vallecula.

Figure 2. Coblator assisted excision of the cyst being done.
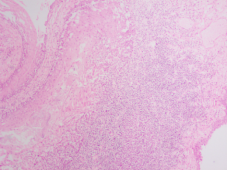
Figure 3. Histopathological appearance, cyst lined by stratified squamous epithelium. Underlying sub epithelium shows dense lymphocytic infiltrate.
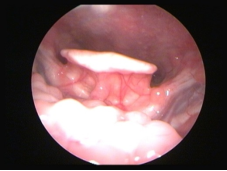
Figure 4. Postoperative endoscopic view showing healed base.

