Background: Spina bifida (SB) is a relatively common birth defect with the highest prevalence among Hispanics. A randomized controlled trial (MOMS) demonstrated that prenatal repair yielded improved outcomes compared to postnatal repair. However, the social determinants of health can significantly impact the overall well-being of affected individuals or their eligibility for some of these evidenced-based interventions. Methods: We conducted a retrospective observational study to describe and compare the mean Child Opportunity Index (COIs) scores among patients treated at a free-standing children’s hospital who underwent either prenatal or postnatal repair of SB from January 1st, 2012, to December 31st, 2021. We excluded patients with identifiable maternal and fetal contraindications to prenatal repair, as per the MOMS trial eligibility, apart from those pertaining to socio-economic status. RESULTS: Among a total cohort of 51 fetuses, 86% (n = 44) underwent postnatal repair for SB, while 14% (n = 7) received prenatal repair. Patients who underwent prenatal repair exhibited lower COI scores across all domains (education, health, and environment, social and economic) on national, state, and metro levels compared to the postnatal group. Our cohort showed a higher percentage of primary commercial insurance in the prenatal (fetal) surgery group (57.14%) versus the postnatal surgery group (47.73%), without attaining statistical significance (p=0.25). Conclusion: While COI scores across all domains were lower in the prenatal cohort, our data does not suggest a statistically significant difference between prenatal and postnatal surgery groups. This highlights the need for future studies with larger sample sizes to further explore and define this relationship.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Spina Bifida, Fetal Surgery, COI, Health Disparities, MMC, Myelomeningocele
1. Introduction
Spina bifida (SB) is a relatively common birth defect, occurring in approximately 1 in 2,500 live births worldwide
[1]
Kancherla V, Wagh K, Johnson Q, Oakley GP, Jr. A 2017 global update on folic acid-preventable spina bifida and anencephaly. Birth Defects Res. 2018; 110: 1139-1147.
. However, its prevalence varies widely depending on geographic location, ethnic group, and other factors. In the United States alone, it is estimated that roughly 1,500 babies are born with SB each year. The prevalence of SB is highest among Hispanics, followed by non-Hispanic Whites and non-Hispanic Blacks
[2]
Mai CT, Isenburg JL, Canfield MA, et al. National population-based estimates for major birth defects, 2010-2014. Birth Defects Res. 2019; 111: 1420-1435.
. Additionally, SB is more common among females than males. SB is a complex condition that can have significant physical, emotional, and social impacts on individuals and their families. While medical interventions can mitigate some of the physical repercussions of SB, the social determinants of health (SDOH) can significantly impact the overall well-being of individuals with this condition. It is estimated that the lifetime cost of care for a person with SB averages around $792,000
[3]
Grosse SD, Berry RJ, Mick Tilford J, Kucik JE, Waitzman NJ. Retrospective Assessment of Cost Savings From Prevention: Folic Acid Fortification and Spina Bifida in the U.S. Am J Prev Med. 2016; 50: S74-S80.
Conventional postnatal repair usually occurs within the first 48 hours of life mainly to prevent infection such as meningitis. Most people with myelomeningocele have hydrocephalus and the majority will need a ventriculoperineal shunt placed as an infant. However, over the last decade, fetal surgery has become increasingly accessible in many countries
[4]
Sacco A, Simpson L, Deprest J, David AL. A study to assess global availability of fetal surgery for myelomeningocele. Prenat Diagn. 2018; 38: 1020-1027.
. In 2011, the groundbreaking MOMS trial demonstrated clear advantages of prenatal repair, including lower rates of shunt placement at 12 months and an enhanced probability of walking without orthotics at 30 months, albeit with a higher risk of preterm birth and maternal uterine dehiscence
[5]
Adzick NS, Thom EA, Spong CY, et al. A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med. 2011; 364: 993-1004.
. Subsequent studies have not only reaffirmed these findings but have also made strides in refining the approach
[15]
Julie S Moldenhauer, N Scott Adzick. Fetal surgery for myelomeningocele: After the Management of Myelomeningocele Study (MOMS). Semin Fetal Neonatal Med. 2017 Dec; 22(6): 360-366.
SDOH encompass the social, economic, and environmental factors that wield influence over an individual's health outcomes. These determinants span factors such as income, education, employment, housing, and access to healthcare. For individuals grappling with SB, these social determinants can significantly impact their quality of life and their capacity to access essential healthcare and support services. Socioeconomic factors are recognized as significant hurdles in medicine, with prenatal SB repair exclusion criteria involving aspects tied to socioeconomic status and resources, including the availability of post-operative support, the ability of support person to travel and stay with patient, the feasibility of temporarily relocating to a new city for fetal surgery, and the capacity to adhere to post-operative care. Given the established advantages of prenatal repair, barriers to such interventions may bear immediate and lifelong health consequences for children born with SB. These consequences are likely even more severe for children born into under-resourced or racial minority families, which are already known to experience worse health outcomes compared to their more privileged counterparts. For instance, Black preterm infants exhibit higher risks than White preterm infants of mortality, sepsis, intracranial hemorrhage, and retinopathy of prematurity; even after controlling for maternal demographic and health factors
[6]
Wallace ME, Mendola P, Kim SS, et al. Racial/ethnic differences in preterm perinatal outcomes. Am J Obstet Gynecol. 2017; 216: 306 e301-306 e312.
. Among children with complex chronic conditions, those residing in neighborhoods in the poorest quintile were more likely than those in the wealthiest quintile to die or be hospitalized in the year after their discharge from neonatal inpatient care
[7]
Wang C, Guttmann A, To T, Dick PT. Neighborhood income and health outcomes in infants: how do those with complex chronic conditions fare? Arch Pediatr Adolesc Med. 2009; 163: 608-615.
. In SB patients under 21 years of age, non-Hispanic Black patients, and patients without private insurance (a marker of high socioeconomic status) were less likely to achieve continence (both urine and stool) compared to patients of other races and those with private insurance. Those with private insurance were also more likely to be ambulatory (with or without orthotic aids) than those with public insurance
[8]
Schechter MS, Liu T, Soe M, Swanson M, Ward E, Thibadeau J. Sociodemographic attributes and spina bifida outcomes. Pediatrics. 2015; 135: e957-964.
. Hispanic and Latino SB patients between the ages of 5 and 21 years were also less likely to have fecal continence than non-Hispanic and non-Latino patients
[9]
Smith KA, Liu T, Freeman KA, et al. Differences in continence rates in individuals with spina bifida based on ethnicity. J Pediatr Rehabil Med. 2019; 12: 361-368.
The Child Opportunity Index (COI) is a measure of the opportunities available to children based on various factors such as education, healthcare, and economic conditions. The COI boasts several advantages, including its enhanced predictive validity, comprehensive measurement of neighborhood quality/resources for children, efficiency, and capacity to better capture racial/ethnic disparities in neighborhood opportunity
[16]
Child Opportunity Index Methodology and Application - CHA Webinar - Dec 2021.pdf.
[16]
. The COI score ranges from 0 to 100, with higher scores indicating greater opportunities for children
[10]
Acevedo-Garcia D, McArdle N, Hardy EF, et al. The child opportunity index: improving collaboration between community development and public health. Health Aff (Millwood). 2014; 33: 1948-1957.
. Neighborhoods are categorized into five groups, each comprising 20% of the child population, based on domain average or overall average z-scores (very low, low, moderate, high, very high; 0-20, 21-40,41-60,61-80,81-100, respectively). The COI v 2.0 which was employed, focuses on neighborhood features pertinent to today’s children, provides granular data on nearly all U.S. neighborhoods (over 72,000 census tracts), offers data that is comparable across neighborhoods and over time (2010, 2015) and demonstrates good predictive validity compared to similar metrics.
Understanding the SDOH in SB becomes paramount in improving the overall well-being of individuals with this condition. By scrutinizing the multifaceted factors influencing health outcomes, researchers, healthcare providers, and policymakers can collaboratively develop interventions and policies to address SDOH and improve outcomes for SB individuals. In this study, we aim to gain a deeper understanding of the relationship between socioeconomic status to choose of surgical repair route—prenatal versus postnatal—and ascertain whether nationally normed indicators of SES, as exemplified by the COI, correlate with the ultimate route of repair.
2. Methods
2.1. Study Participants and Design
A retrospective observational study was conducted with the aim of comparing the mean COI scores among patients followed in the Spina Bifida Clinic at Nationwide Children’s Hospital (NCH) who underwent either prenatal or postnatal repair of SB. Inclusion criteria consisted of all new patients diagnosed with SB (Q05.9) at NCH’s Spina Bifida Clinic who underwent either postnatal or prenatal repair from January 1st, 2012, to December 31st, 2021. We excluded patients with diagnoses of SB occulta, chromosomal anomalies, or syndromic conditions. Additionally, patients with contraindications to prenatal repair, as specified by the MOM's trial eligibility criteria, were also excluded. These contraindications encompassed factors such as maternal insulin-dependent pregestational diabetes, short cervix, cervical cerclage, placenta previa, body mass index (BMI) of 35 or more, previous spontaneous delivery prior to 37 weeks, maternal HIV, hepatitis B or hepatitis C positivity, uterine anomaly, maternal medical contraindications to surgery or general anesthesia, or other fetal anomalies. The Institutional Review Board at NCH reviewed and approved this retrospective study. Among the 121 patients with a prenatal SB diagnosis, 12 declined participation in research studies, 56 did not meet the inclusion criteria, and data for 2 patients were incomplete.
2.2. Measure of Interest
Community-level determinants of health, such as neighborhood resources and living conditions that affect children, are captured in the COI. The COI compiles a composite index at the census tract level. Data for the COI were collected in 2010 and again in 2015. COI scores provide indications of features within the neighborhood that can be applied to helping children develop in a healthy manner. COI scores are nationally normed and range from 1 to 100 with lower scores indicating low opportunity for a child and higher scores indicating higher opportunity.
2.3. Data Collection
Census tract data for each patient in 2015 were matched with publicly available COI data from the COI2.0 database using unique geographic identifiers (GEOIDs) assigned by the US Census Bureau. This dataset included indices for three domains: educational opportunity, health and environmental opportunity, and social and economic opportunity, with a total of 29 indicators. Subgroups within the education domain include early childhood education, elementary education, secondary and postsecondary education, and educational and social resources. Subgroups within the health and environment domain include healthy environments, toxic exposures, and health resources. Subgroups within the social and economic domain included economic opportunities and economic and social resources. Metro, state, and national normed Z-scores for each domain was utilized.
2.4. Independent Variables
Fetal characteristics were extracted manually from review of the electronic medical records and compiled for analyses. These characteristics included fetal race, gestational age, birth weight, birth length, and presence of the following indications: ventriculomegaly, hindbrain herniation (Chiari II malformation), club feet, age when the repair was conducted, NICU length of stay, age at initial myelomeningocele visit, no show rate, and whether the patient resided in one of the 100 largest metropolitan areas. Maternal characteristics included all demographic information, as well as delivery details such as delivery type, prior C-sections, nulliparity, and access to transport.
2.5. Statistical Analysis
Descriptive analyses were conducted, presenting categorical data as counts and proportions, while continuous data were described using mean and standard deviation for parametric data and median and interquartile range for non-parametric data. Normality distribution was assessed through histograms, QQ plots, skewness, kurtosis, and the Shapiro-Wilk test. Bivariate analyses employed Chi-square or Fisher's exact tests for categorical variables and T-tests or Wilcoxon tests for parametric and non-parametric continuous data, respectively. Generalized linear model using the identity link function was used to estimate mean COI scores as well as differences in scores between postnatal and prenatal repair types. Findings were determined to be statistically significant at p < 0.05. All statistical tests were conducted using SAS Enterprise version 8.1 and Stata 16.0. Figures drafted looking at COI scores by domain among both prenatal and postnatal repair type were conducted on Microsoft Excel 365.
3. Results
3.1. Participant Characteristics
Out of a total cohort of 51 fetuses, 86% (n = 44) had postnatal repair for SB while 14% (n = 7) had repair performed prenatally. The median gestational age at birth was 266 days (IQR 259, 274) and mean birth weight was 3204.5 grams (SD = 590.63). A total of 32 (63%) of patients were diagnosed with ventriculomegaly, 39 (76%) with hindbrain herniation (Chiari II malformation), and 17 (33%) were observed to have club feet. Patients who received postnatal repair were born, understandably at a significantly higher gestational age, with a median age of 269.5 days (IQR 264, 274), compared to 243 days (IQR 223, 259) for those who received prenatal repair (p = 0.0001). Postnatal repair was performed at a median age of 1 day (IQR 1, 1) while patients who received prenatal repair had it performed at a median gestational age of 24 weeks and 6 days. Other fetal characteristics did not significantly differ between the two repair groups (p > 0.05). Similarly, there were no significant differences in maternal characteristics between the repair groups (p > 0.05) (Table 1).
3.2. Child Opportunity Index (COI) Scores
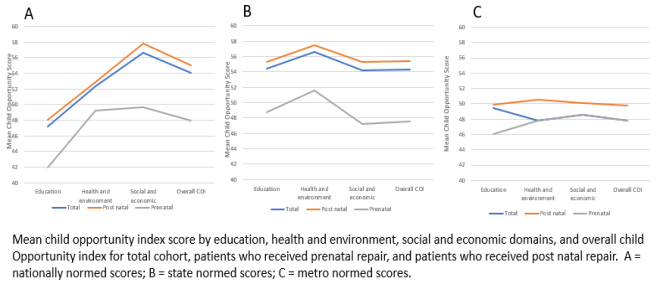
Overall, patients who received prenatal repair had lower COI scores across all domains on national, state, and metro levels. Differences in COI scores between both patient groups were more minimized when examined on a metropolitan level (Figure 1).
3.2.1. National Level Analysis
COI scores among all domains did not differ significantly between the postnatal and prenatal groups (P > 0.05) on a national level. On a national scale, COI scores for patients who received postnatal repair were higher than those who received prenatal repair by 6.05 points (95% CI [-14.11, 26.2]) among the education domain, 3.58 points (95% CI [-14.58, 21.74]) among the health and environment domain, 8.08 points (95% CI [-15.83, 31.99]) among the social and economic domain, and 7 points (95% CI [-15.35, 29.35]) for the overall COI domain. Findings did not indicate statistical differences between both repair groups, however (p > 0.05) (Table 2).
3.2.2. State Level Analysis
Similarly, COI scores at the state level did not differ significantly between patients who underwent postnatal repair and those who underwent prenatal repair (p > 0.05). On average, patients in the postnatal repair group had slightly higher COI scores compared to the prenatal repair group: 6.65 points higher (95% CI [-13.66, 26.95]) in the education domain, 5.91 points higher (95% CI [-15.61, 27.43]) in the health and environment domain, 8 points higher (95% CI [-14.59, 30.57]) in the social and economic domain, and 7.84 points higher (95% CI [-14.27, 29.94]) in the overall COI domain (Table 2).
3.2.3. Metropolitan Level Analysis
At the metropolitan level, COI scores did not show significant differences between patients in both repair groups (p > 0.05). However, estimate differences between patients of both repair types were smaller in scale compared to national and state levels. Compared to patients who had prenatal repairs, patients who received postnatal repairs on average had 3.29 points higher (95% CI [-19.63, 26.22]) among the education domain, 2.7 points (95% CI [-25.03, 30.43]) among the health and environment domain, 1.51 points (95% CI [-26.1, 29.11]) among the social and economic domain, and 2.02 points (95% CI [-24.51, 28.55]) among the overall COI domain (Table 2).
Table 1. Fetal and maternal characteristics among spina bifida patients by type of repair.
Repair
Total
Postnatal
Prenatal
n = 51
n = 44
n = 7
100%
86.27%
13.73%
Characteristic
n (%)
n (%)
n (%)
P value
Fetal
Race
White
43 (84.31)
37 (84.09)
6 (85.71)
0.722
Black
5 (9.8)
4 (9.09)
1 (14.29)
Multiracial
2 (3.92)
2 (4.55)
0 (0)
Asian
1 (1.96)
1 (2.27)
0 (0)
Gestational age at birth, d, median (IQR)
266 (259, 274)
269.5 (264, 274)
243 (223, 259)
0.0001
Birth weight, g, mean (SD)
3204.53 (590.63)
3297.70 (439.89)
2618.86 (1027.83)
0.133
Birth length, cm, mean (SD)
48.02 (3.47)
48.56 (2.82)
44.69 (5.23)
0.0994
Ventriculomegaly (at presentation)
32 (62.75)
25 (56.82)
7 (100)
0.028
Hindbrain Herniation (Chiari) (at presentation)
41 (80.39)
34 (77.27)
7 (100)
0.160
Club Feet
17 (33.33)
13 (29.55)
4 (57.14)
0.203
Resides in one of the 100 largest metro areas
33 (70.21)
28 (70)
5 (71.43)
1
Age at repair, d, median (IQR)
1 (1, 1)
Gestational age at prenatal repair, d, median (IQR)
24w6d (24w4d, 25w3d)
NICU length of stay, d, median (IQR)
15 (11, 21)
13.5 (11, 20)
19 (6, 27)
0.6026
Initial postnatal follow-up visit age, d, median (IQR)
30 (23, 46)
29 (23.5, 46)
30 (22, 51)
0.8159
No show rate, median (IQR)
0.03 (0.01, 0.06)
0.03 (0.01, 0.07)
0.03 (0.01, 0.06)
0.8997
Maternal
Race
White
45 (88.24)
39 (88.64)
6 (85.71)
1
Black
6 (11.76)
5 (11.36)
1 (14.29)
Non-Hispanic
51 (100)
44 (100)
7 (100)
-
Delivery type
Cesarian
47 (92.16)
40 (90.91)
7 (100)
1
Vaginal
4 (7.84)
4 (9.09)
0 (0)
Prior C-section (n = 28)
7 (25)
7 (28)
0 (0)
0.551
Nulliparity
18 (35.29)
15 (34.09)
3 (42.86)
0.686
Initial insurance
Commercial
25 (49.02)
21 (47.73)
4 (57.14)
0.251
Medicaid
24 (47.06)
22 (50)
2 (28.57)
Other (Tricare)
2 (3.92)
1 (2.27)
1 (14.29)
Insurance at discharge
Public
26 (50.98)
24 (54.55)
2 (28.57)
0.261
Private
20 (39.22)
15 (34.09)
5 (71.43)
Combined
5 (9.8)
5 (11.36)
0 (0)
Access to transportation
48 (94.12)
41 (93.18)
7 (100)
1
D = Days; IQR = Interquartile range; g = Grams; SD = Standard deviation
Table 2. Mean child opportunity index scores among spina bifida patients who received either postnatal or prenatal repair.
Figure 1. Nationally normed (A), state normed (B), and metro normed (C) child opportunity scores among all spina bifida patients who received either postnatal or prenatal repair in the NCH Myelomeningocele clinic from January 1, 2012 to December 31, 2021.
4. Discussion
4.1. Main Findings
The study revealed that there is no statistically significant difference in socioeconomic status, as indicated by the Childhood Opportunity Index (COI), between prenatal and postnatal repair cohorts in our subject population. A higher percentage of prenatal patients had private insurance compared to public insurance. However, patients who received prenatal repair in general had lower COI scores across all domains on national, state, and metro levels. Interestingly, the differences in COI scores between both patient groups were less pronounced when examined at the metropolitan level alone.
4.2. Interpretation of Results
The cohort demonstrated a higher percentage of initially reported primary commercial insurance in the prenatal (fetal) surgery group (57.14%) compared to the postnatal surgery group (47.73%), although this difference was not statistically significant (p=0.25). Additionally, at discharge, a higher percentage of patients with public insurance underwent postnatal repair (54.55%) compared with those with prenatal repair (28.57%), although this difference also did not attain statistical significance (p=0.26).
The association between prenatal surgery and private insurance status can be rationalized by the increased costs associated with relocation, travel to imaging centers and fetal care offices, and childcare, which are often deemed as "medically unnecessary care" and may not be covered by insurance providers. As such, it is logical to associate prenatal repair groups with private insurance to accommodate for the higher expenses associated with prenatal repair. Indeed, Foy et al. showed a positive correlation between private insurance status and fetal surgery
[11]
Foy AB, Sawin KJ, Derflinger T, et al. Sociodemographic disparities in fetal surgery for myelomeningocele: a single-center retrospective review. J Neurosurg Pediatr. 2021: 1-5.
. Fabelo et. al. also found that between prenatal and postnatal patients, there were significant differences in influence of insurance coverage and costs of relocation and travel on the choice of procedure. Specifically, postnatal patients reported more influence from associated costs and less influence from insurance coverage of the procedure, with higher influence in respondents with Medicaid
[12]
Fabelo C, He H, Lim FY, Atzinger C, Wong B. Factors impacting surgical decision making between prenatal and postnatal repair for myelomeningocele. Prenat Diagn. 2022; 42: 27-36.
. More so, the role of costs in this cohort of patients, who were overwhelmingly postnatal, could not be over emphasized given, the universal need to relocate outside of the city to avail of opportunities of prenatal surgical interventions. These findings match what has been found in the literature to date, regarding insurance status and choice of repair in SB.
This study introduces the novel use of the COI as a surrogate for socioeconomic status in the context of maternal-fetal surgery. Although findings did not rise to the level of statistical significance, the COI revealed the prenatal surgery cohort had slightly lower scores across all domains. While the data is limited by a small sample size, this finding is contrary to the expectation that higher socioeconomic status would be associated with prenatal repair for SB. Especially given the premise that lower COI scores are associated with limited access to care and consequently associated surgical procedures, particularly those as involving as fetal surgery. The discrepancy may be due to a subset of patients who underwent prenatal repair outside of region and continued to receive postnatal care outside of network, possibly representing a more affluent group that wasn't captured by local spina bifida clinic data. Additionally, the disparity in this study findings of the association of low COI with prenatal repair, compared to some earlier studies, may be an unlikely reflection of minimal capture of true socioeconomic variables in studies involving Maternal-Fetal surgery as alluded to in a recent study
[13]
Wilpers A, Lynn AY, Eichhorn B, et al. Understanding Sociodemographic Disparities in Maternal-Fetal Surgery Study Participation. Fetal Diagn Ther. 2022; 49: 125-137.
Few prior studies have specifically examined the sociodemographic characteristics of myelomeningocele patients beyond insurance coverage. The MOMs trial showed patients in the fetal surgery cohort had a higher degree of social stability, racial homogeneity, and higher education. Additionally, Wilpers et. al. examined 112 maternal-fetal surgery studies and found extremely poor quality of sociodemographic reporting among MMC disease groups
[13]
Wilpers A, Lynn AY, Eichhorn B, et al. Understanding Sociodemographic Disparities in Maternal-Fetal Surgery Study Participation. Fetal Diagn Ther. 2022; 49: 125-137.
Harbert et. al., recently published findings suggesting that an additional unmeasured social factor may affect the relationship between insurance status and eligibility for open maternal fetal surgery. In their study, fetal surgery cohorts were found to be homogenous and not representative of the total population of patients affected by SB. They also found Medicaid or uninsured status were significantly associated with ineligibility for OMFS, despite insurance status not being considered in determining eligibility
[14]
Harbert AL, Barnett RR, Abumoussa AL, Goodnight WH, Tolleson-Rinehart S, Quinsey CS. Sociodemographic disparities as a determinant of fetal versus postnatal surgical myelomeningocele repair. J Neurosurg Pediatr. 2022: 1-7.
. With the patient cohort showing a disparity between insurance status and a proven index of socioeconomic status between prenatal and postnatal surgical groups, vis-à-vis insurance type, it contributes additional data to the literature that questions how accurately insurance type can be used as a surrogate for socioeconomic status. It therefore remains unknown whether patients with fetal repair of myelomeningocele have underlying socioeconomic differences that may contribute to post-surgical outcomes. Further research with increased prenatal cohort sizes is needed to answer this question.
4.3. Strengths and Limitations
The main strength of this study is the use of the COI as a standardized measurement for SDOH. The scores used in the COI can capture a wide variety of social and economic factors that offer significantly more information compared to the commonly used surrogate of SDOH, insurance type. Additionally, since these scores are metro, state, and nationally normed, our data can be extrapolated to the general US population and, although not perfect, is more representative of population of interest than prior studies.
However, thisstudy also has limitations, including its retrospective single-center design and small sample size. This institution does not yet have the number of operations needed to supply a robust prenatal cohort size. This is more telling among the prenatal surgery cohort, which were underrepresented given the erstwhile unavailability of Fetal intervention prior to establishment of the fetal center. Additionally, multiple patients were excluded due to non-participation in research and inability to obtain certain variables from the retrospective chart review.
5. Conclusion
In conclusion, although COI scores across all domains were lower in the prenatal cohort, our data did not demonstrate a statistically significant difference between prenatal and postnatal surgery groups. The small sample size likely influenced these results, highlighting the need for future studies with larger cohorts to further investigate and define the relationship between socioeconomic status and the choice of repair for Spina Bifida.
Ethics Approval
This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The Human Investigation Committee (IRB) of Nationwide Children’s Hospital approved this study.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Oluseyi Ogunleye and Jason Xia. All authors read and approved the final manuscript.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Kancherla V, Wagh K, Johnson Q, Oakley GP, Jr. A 2017 global update on folic acid-preventable spina bifida and anencephaly. Birth Defects Res. 2018; 110: 1139-1147.
Mai CT, Isenburg JL, Canfield MA, et al. National population-based estimates for major birth defects, 2010-2014. Birth Defects Res. 2019; 111: 1420-1435.
Grosse SD, Berry RJ, Mick Tilford J, Kucik JE, Waitzman NJ. Retrospective Assessment of Cost Savings From Prevention: Folic Acid Fortification and Spina Bifida in the U.S. Am J Prev Med. 2016; 50: S74-S80.
Sacco A, Simpson L, Deprest J, David AL. A study to assess global availability of fetal surgery for myelomeningocele. Prenat Diagn. 2018; 38: 1020-1027.
Wang C, Guttmann A, To T, Dick PT. Neighborhood income and health outcomes in infants: how do those with complex chronic conditions fare? Arch Pediatr Adolesc Med. 2009; 163: 608-615.
Smith KA, Liu T, Freeman KA, et al. Differences in continence rates in individuals with spina bifida based on ethnicity. J Pediatr Rehabil Med. 2019; 12: 361-368.
Acevedo-Garcia D, McArdle N, Hardy EF, et al. The child opportunity index: improving collaboration between community development and public health. Health Aff (Millwood). 2014; 33: 1948-1957.
Foy AB, Sawin KJ, Derflinger T, et al. Sociodemographic disparities in fetal surgery for myelomeningocele: a single-center retrospective review. J Neurosurg Pediatr. 2021: 1-5.
Fabelo C, He H, Lim FY, Atzinger C, Wong B. Factors impacting surgical decision making between prenatal and postnatal repair for myelomeningocele. Prenat Diagn. 2022; 42: 27-36.
Wilpers A, Lynn AY, Eichhorn B, et al. Understanding Sociodemographic Disparities in Maternal-Fetal Surgery Study Participation. Fetal Diagn Ther. 2022; 49: 125-137.
Julie S Moldenhauer, N Scott Adzick. Fetal surgery for myelomeningocele: After the Management of Myelomeningocele Study (MOMS). Semin Fetal Neonatal Med. 2017 Dec; 22(6): 360-366.
Ogunleye, O., Xia, J., Cruz, S., Saulsbery, A., Nicoll, R., et al. (2024). Health Disparities and Route of Repair of Fetal Myelomeningocele-Prenatal Versus Postnatal Repair. Advances in Surgical Sciences, 12(1), 27-35. https://doi.org/10.11648/j.ass.20241201.15
Ogunleye, O.; Xia, J.; Cruz, S.; Saulsbery, A.; Nicoll, R., et al. Health Disparities and Route of Repair of Fetal Myelomeningocele-Prenatal Versus Postnatal Repair. Adv. Surg. Sci.2024, 12(1), 27-35. doi: 10.11648/j.ass.20241201.15
Ogunleye O, Xia J, Cruz S, Saulsbery A, Nicoll R, et al. Health Disparities and Route of Repair of Fetal Myelomeningocele-Prenatal Versus Postnatal Repair. Adv Surg Sci. 2024;12(1):27-35. doi: 10.11648/j.ass.20241201.15
@article{10.11648/j.ass.20241201.15,
author = {Oluseyi Ogunleye and Jason Xia and Stephanie Cruz and Angela Saulsbery and Ryan Nicoll and Amy Schlegel and Adolfo Etchegaray and Eric Sribnick and Oluyinka Olutoye},
title = {Health Disparities and Route of Repair of Fetal Myelomeningocele-Prenatal Versus Postnatal Repair
},
journal = {Advances in Surgical Sciences},
volume = {12},
number = {1},
pages = {27-35},
doi = {10.11648/j.ass.20241201.15},
url = {https://doi.org/10.11648/j.ass.20241201.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ass.20241201.15},
abstract = {Background: Spina bifida (SB) is a relatively common birth defect with the highest prevalence among Hispanics. A randomized controlled trial (MOMS) demonstrated that prenatal repair yielded improved outcomes compared to postnatal repair. However, the social determinants of health can significantly impact the overall well-being of affected individuals or their eligibility for some of these evidenced-based interventions. Methods: We conducted a retrospective observational study to describe and compare the mean Child Opportunity Index (COIs) scores among patients treated at a free-standing children’s hospital who underwent either prenatal or postnatal repair of SB from January 1st, 2012, to December 31st, 2021. We excluded patients with identifiable maternal and fetal contraindications to prenatal repair, as per the MOMS trial eligibility, apart from those pertaining to socio-economic status. RESULTS: Among a total cohort of 51 fetuses, 86% (n = 44) underwent postnatal repair for SB, while 14% (n = 7) received prenatal repair. Patients who underwent prenatal repair exhibited lower COI scores across all domains (education, health, and environment, social and economic) on national, state, and metro levels compared to the postnatal group. Our cohort showed a higher percentage of primary commercial insurance in the prenatal (fetal) surgery group (57.14%) versus the postnatal surgery group (47.73%), without attaining statistical significance (p=0.25). Conclusion: While COI scores across all domains were lower in the prenatal cohort, our data does not suggest a statistically significant difference between prenatal and postnatal surgery groups. This highlights the need for future studies with larger sample sizes to further explore and define this relationship.
},
year = {2024}
}
TY - JOUR
T1 - Health Disparities and Route of Repair of Fetal Myelomeningocele-Prenatal Versus Postnatal Repair
AU - Oluseyi Ogunleye
AU - Jason Xia
AU - Stephanie Cruz
AU - Angela Saulsbery
AU - Ryan Nicoll
AU - Amy Schlegel
AU - Adolfo Etchegaray
AU - Eric Sribnick
AU - Oluyinka Olutoye
Y1 - 2024/06/14
PY - 2024
N1 - https://doi.org/10.11648/j.ass.20241201.15
DO - 10.11648/j.ass.20241201.15
T2 - Advances in Surgical Sciences
JF - Advances in Surgical Sciences
JO - Advances in Surgical Sciences
SP - 27
EP - 35
PB - Science Publishing Group
SN - 2376-6182
UR - https://doi.org/10.11648/j.ass.20241201.15
AB - Background: Spina bifida (SB) is a relatively common birth defect with the highest prevalence among Hispanics. A randomized controlled trial (MOMS) demonstrated that prenatal repair yielded improved outcomes compared to postnatal repair. However, the social determinants of health can significantly impact the overall well-being of affected individuals or their eligibility for some of these evidenced-based interventions. Methods: We conducted a retrospective observational study to describe and compare the mean Child Opportunity Index (COIs) scores among patients treated at a free-standing children’s hospital who underwent either prenatal or postnatal repair of SB from January 1st, 2012, to December 31st, 2021. We excluded patients with identifiable maternal and fetal contraindications to prenatal repair, as per the MOMS trial eligibility, apart from those pertaining to socio-economic status. RESULTS: Among a total cohort of 51 fetuses, 86% (n = 44) underwent postnatal repair for SB, while 14% (n = 7) received prenatal repair. Patients who underwent prenatal repair exhibited lower COI scores across all domains (education, health, and environment, social and economic) on national, state, and metro levels compared to the postnatal group. Our cohort showed a higher percentage of primary commercial insurance in the prenatal (fetal) surgery group (57.14%) versus the postnatal surgery group (47.73%), without attaining statistical significance (p=0.25). Conclusion: While COI scores across all domains were lower in the prenatal cohort, our data does not suggest a statistically significant difference between prenatal and postnatal surgery groups. This highlights the need for future studies with larger sample sizes to further explore and define this relationship.
VL - 12
IS - 1
ER -
The Fetal Center, Nationwide Children’s Hospital, Columbus, The United States; Department of Maternal Fetal Medicine, Nationwide Children’s Hospital, Columbus, The United States
Department of Surgery, Nationwide Children’s Hospital, Columbus, The United States; Department of Regenerative Medicine, Abigail Wexner Research Institute, Nationwide Children’s Hospital, Columbus, The United States
Stephanie Cruz
The Fetal Center, Nationwide Children’s Hospital, Columbus, The United States; Department of Surgery, Nationwide Children’s Hospital, Columbus, The United States
The Fetal Center, Nationwide Children’s Hospital, Columbus, The United States
Amy Schlegel
Department of Pediatrics, The Ohio State University School of Medicine, Columbus, The United States; Division of Neonatology, Nationwide Children’s Hospital, Columbus, The United States
Department of Regenerative Medicine, Abigail Wexner Research Institute, Nationwide Children’s Hospital, Columbus, The United States; Department of Neurosurgery, Nationwide Children’s Hospital, Columbus, The United States; Department of Neurosurgery, The Ohio State University College of Medicine, Columbus, The United States
The Fetal Center, Nationwide Children’s Hospital, Columbus, The United States; Department of Surgery, Nationwide Children’s Hospital, Columbus, The United States; Department of Regenerative Medicine, Abigail Wexner Research Institute, Nationwide Children’s Hospital, Columbus, The United States; Department of Surgery, The Ohio State University College of Medicine, Columbus, The United States
Ogunleye, O., Xia, J., Cruz, S., Saulsbery, A., Nicoll, R., et al. (2024). Health Disparities and Route of Repair of Fetal Myelomeningocele-Prenatal Versus Postnatal Repair. Advances in Surgical Sciences, 12(1), 27-35. https://doi.org/10.11648/j.ass.20241201.15
Ogunleye, O.; Xia, J.; Cruz, S.; Saulsbery, A.; Nicoll, R., et al. Health Disparities and Route of Repair of Fetal Myelomeningocele-Prenatal Versus Postnatal Repair. Adv. Surg. Sci.2024, 12(1), 27-35. doi: 10.11648/j.ass.20241201.15
Ogunleye O, Xia J, Cruz S, Saulsbery A, Nicoll R, et al. Health Disparities and Route of Repair of Fetal Myelomeningocele-Prenatal Versus Postnatal Repair. Adv Surg Sci. 2024;12(1):27-35. doi: 10.11648/j.ass.20241201.15
@article{10.11648/j.ass.20241201.15,
author = {Oluseyi Ogunleye and Jason Xia and Stephanie Cruz and Angela Saulsbery and Ryan Nicoll and Amy Schlegel and Adolfo Etchegaray and Eric Sribnick and Oluyinka Olutoye},
title = {Health Disparities and Route of Repair of Fetal Myelomeningocele-Prenatal Versus Postnatal Repair
},
journal = {Advances in Surgical Sciences},
volume = {12},
number = {1},
pages = {27-35},
doi = {10.11648/j.ass.20241201.15},
url = {https://doi.org/10.11648/j.ass.20241201.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ass.20241201.15},
abstract = {Background: Spina bifida (SB) is a relatively common birth defect with the highest prevalence among Hispanics. A randomized controlled trial (MOMS) demonstrated that prenatal repair yielded improved outcomes compared to postnatal repair. However, the social determinants of health can significantly impact the overall well-being of affected individuals or their eligibility for some of these evidenced-based interventions. Methods: We conducted a retrospective observational study to describe and compare the mean Child Opportunity Index (COIs) scores among patients treated at a free-standing children’s hospital who underwent either prenatal or postnatal repair of SB from January 1st, 2012, to December 31st, 2021. We excluded patients with identifiable maternal and fetal contraindications to prenatal repair, as per the MOMS trial eligibility, apart from those pertaining to socio-economic status. RESULTS: Among a total cohort of 51 fetuses, 86% (n = 44) underwent postnatal repair for SB, while 14% (n = 7) received prenatal repair. Patients who underwent prenatal repair exhibited lower COI scores across all domains (education, health, and environment, social and economic) on national, state, and metro levels compared to the postnatal group. Our cohort showed a higher percentage of primary commercial insurance in the prenatal (fetal) surgery group (57.14%) versus the postnatal surgery group (47.73%), without attaining statistical significance (p=0.25). Conclusion: While COI scores across all domains were lower in the prenatal cohort, our data does not suggest a statistically significant difference between prenatal and postnatal surgery groups. This highlights the need for future studies with larger sample sizes to further explore and define this relationship.
},
year = {2024}
}
TY - JOUR
T1 - Health Disparities and Route of Repair of Fetal Myelomeningocele-Prenatal Versus Postnatal Repair
AU - Oluseyi Ogunleye
AU - Jason Xia
AU - Stephanie Cruz
AU - Angela Saulsbery
AU - Ryan Nicoll
AU - Amy Schlegel
AU - Adolfo Etchegaray
AU - Eric Sribnick
AU - Oluyinka Olutoye
Y1 - 2024/06/14
PY - 2024
N1 - https://doi.org/10.11648/j.ass.20241201.15
DO - 10.11648/j.ass.20241201.15
T2 - Advances in Surgical Sciences
JF - Advances in Surgical Sciences
JO - Advances in Surgical Sciences
SP - 27
EP - 35
PB - Science Publishing Group
SN - 2376-6182
UR - https://doi.org/10.11648/j.ass.20241201.15
AB - Background: Spina bifida (SB) is a relatively common birth defect with the highest prevalence among Hispanics. A randomized controlled trial (MOMS) demonstrated that prenatal repair yielded improved outcomes compared to postnatal repair. However, the social determinants of health can significantly impact the overall well-being of affected individuals or their eligibility for some of these evidenced-based interventions. Methods: We conducted a retrospective observational study to describe and compare the mean Child Opportunity Index (COIs) scores among patients treated at a free-standing children’s hospital who underwent either prenatal or postnatal repair of SB from January 1st, 2012, to December 31st, 2021. We excluded patients with identifiable maternal and fetal contraindications to prenatal repair, as per the MOMS trial eligibility, apart from those pertaining to socio-economic status. RESULTS: Among a total cohort of 51 fetuses, 86% (n = 44) underwent postnatal repair for SB, while 14% (n = 7) received prenatal repair. Patients who underwent prenatal repair exhibited lower COI scores across all domains (education, health, and environment, social and economic) on national, state, and metro levels compared to the postnatal group. Our cohort showed a higher percentage of primary commercial insurance in the prenatal (fetal) surgery group (57.14%) versus the postnatal surgery group (47.73%), without attaining statistical significance (p=0.25). Conclusion: While COI scores across all domains were lower in the prenatal cohort, our data does not suggest a statistically significant difference between prenatal and postnatal surgery groups. This highlights the need for future studies with larger sample sizes to further explore and define this relationship.
VL - 12
IS - 1
ER -